
Key Takeaways
-
Autologous fat grafting and liposuction harvest are still commonplace but are not without limitations including variable graft survival and donor site morbidity. Clinicians need to balance the risks and have honest expectations with patients.
-
Synthetic fat graft, which sought to imitate real adipose tissue and provide standardized volume with reduced necrosis risk and less invasive harvesting, presents a functional option when donor fat is scarce.
-
When selecting products, clinicians can monitor advances in material science, biocompatibility, and engineering that enhance scaffold structure, vascular integration and customizable graft properties.
-
Early clinical data demonstrates encouraging graft retention and safety for synthetic alternatives. Providers should consider trial results and long-term outcomes prior to widespread use.
-
Patient experience is better with synthetic grafts due to shorter recovery, no donor-site scarring, and more predictable cosmetic results. Incorporate patient education and personalized planning into consultations.
-
Regulatory approval, standardized testing and manufacturing quality control still represent major hurdles. Adhere to regulatory guidelines and insist on strong safety data prior to incorporating emerging synthetic graft technologies.
Synthetic fat graft future replacing liposuction harvest, or lab-made fat that replaces fat harvested from a patient by liposuction.
Scientists are striving to create grafts that mimic actual fat in feel, vascularization, and durability. Early trials demonstrate controlled expansion and less donor-site morbidity.
Regulatory, cost, and long-term safety concerns persist. The remainder of the paper covers existing techniques, trial outcomes, and realistic timeframes for clinical adoption.
The Current Standard
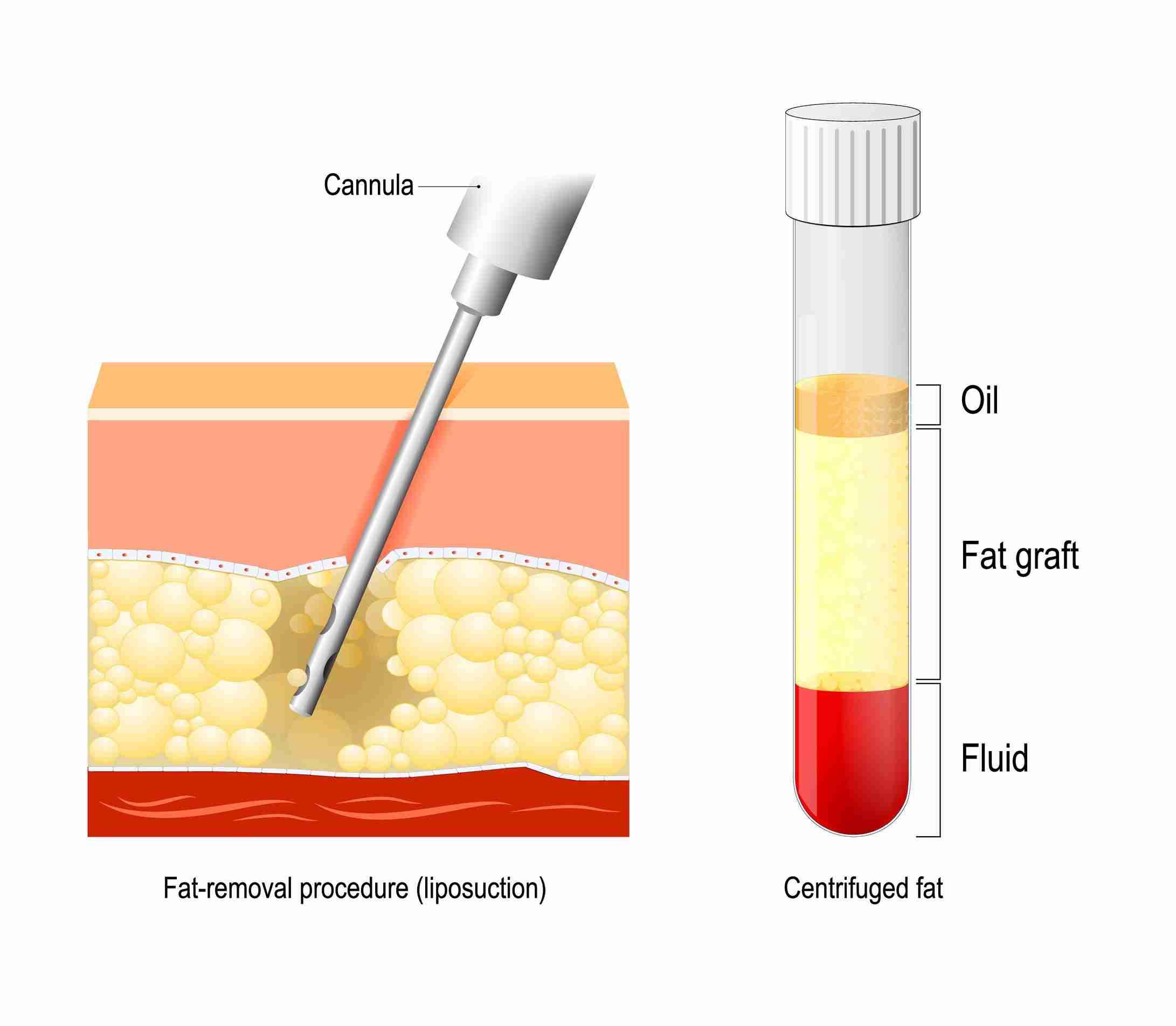
Autologous fat grafting and conventional liposuction harvest continues to be the gold standard for adipose tissue acquisition in cosmetic and reconstructive surgery. Surgeons typically use the Coleman technique as the baseline protocol: gentle aspiration with small cannulas, centrifugation purification, and micro-aliquot injection. The process tries to maintain cell viability at harvest, drain oils and blood, and inject tiny aliquots of fat for better survival.
Current purification standards require centrifuging at approximately 3,000 rpm for three minutes. This action eliminates non-viable substance and consolidates healthy fat cells and stromal cells. Post-centrifugation, clinicians adhere to tissue biology-driven micro-aliquot injection guidelines. Studies show necrotic tissue starts around 0.6 mm from the fat particle boundary, so surgeons section grafts into small bundles to maintain cells proximal to recipient vasculature and reduce central necrosis.
Fat graft survival is inconsistent, with clinical data demonstrating average retention of 50 to 70 percent at one year. Factors that influence this are harvest technique, handling, recipient site vascularity, and the size of each deposit. To maximize contact with capillaries, the standard injection volume per deposit is 0.1 to 0.5 mL in multiple tissue planes. NIH clinical guidelines echo this micro-aliquot approach and suggest depositing those small volumes per pass to minimize pressure on tissue and enhance integration.
Harvest technique is different from traditional liposuction in important respects. For grafting, cell viability is the priority. Surgeons use smaller, approximately 3 mm cannulas and lower suction pressures to minimize mechanical trauma. Regular liposuction, in contrast, emphasizes volume removal efficiency and frequently employs larger cannulas and more powerful suction that can rupture cells if those tissues were to be used for grafting.
Donor site morbidity tends to be lower when surgeons minimize trauma. However, harvest still poses risk for contour irregularity, infection, and transient numbness. Unlike synthetic fillers and implants, autologous fat provides viable, living tissue that can assimilate and evolve with the body. Fillers provide dependable short-term quantities and not long-term sustainability.
Implants provide a firm foundation but necessitate an alien substance and harbor specific dangers. Fat transfer recovery usually includes mild swelling and bruising at donor and recipient sites, with most facial sessions harvesting 70 to 180 mL of fat and customizing micro-aliquot placement to each anatomic zone.
Common applications for harvested fat include:
-
Facial volume restoration and contouring
-
Breast reconstruction and augmentation
-
Gluteal augmentation
-
Scar revision and soft tissue defects
-
Hand rejuvenation and tendon coverage
Synthetic Grafts
Synthetic fat grafts that recapitulate important physical and biological characteristics of native adipose tissue yet circumvent the need for liposuction harvest. They provide predictable volume, structural support, and a scaffold for tissue ingrowth. With no direct clinical facts mentioned in the provided context about synthetic grafts, this section relies on basic material science and translational principles, acknowledging gaps in evidence.
1. Material Science
Synthetic grafts use a range of biomaterials, including porous polymer scaffolds, hydrogels, and composite matrices that combine synthetic and natural polymers. Examples include polycaprolactone (PCL) scaffolds, polyethylene glycol (PEG) hydrogels, and collagen-coated matrices.
These materials differ in elasticity, porosity, and degradation rate, which determines how well they hold shape and allow for cell and vessel in-growth. Material advances enhance graft retention by matching scaffold stiffness with native fat and by customizing pore size to support adipocyte survival and capillary formation.
Scaffold architecture mediates nutrient convection and common pore sizes of 100 to 300 micrometers support vascular ingrowth. Materials can either harbor instructive signals or be seeded with cells to accelerate integration. Scaffold structure is central: a stable yet porous scaffold supports adipocyte viability and new blood vessel formation.
Without vascularization, the central graft regions are at risk for necrosis. Hence, it is imperative to design the scaffold to strike the balance between mechanical support and room for vessels.
|
Property |
Synthetic grafts (typical) |
Autologous fat |
|---|---|---|
|
Elasticity |
Tunable (soft to moderate) |
Native tissue elasticity |
|
Porosity |
Controlled, interconnected |
Variable, cell-packed |
|
Integration |
Designed for guided ingrowth |
Depends on revascularization |
|
Volume consistency |
High |
Variable, resorption common |
2. Biocompatibility
Biocompatibility is key to avoid an immune reaction and to maximize graft take. Current synthetic grafts utilize inert backbones or bioactive molecule coatings to minimize inflammation and restrict graft necrosis. They can incorporate anti-inflammatory agents or peptides that promote host cell adhesion.
Materials that support neovascularization encourage stable integration with native adipose tissue. Research in analogous synthetic implants demonstrates decreased fibrosis when materials are aligned with host mechanics. Direct clinical data for synthetic fat grafting is sparse.
As reported, fat grafting with autologous tissue has well-known survival ranges. Synthetic analogs require equivalent data.
3. Engineering
Engineering allows us to tune particle size, internal channels, and graft volume. 3D printing and microfabrication could reproduce adipose lobule geometry and vessel channels. Nanotechnology provides surface textures that enhance cell adhesion.
Delivery systems seek accuracy and low tissue trauma. Aims to improve cell survival, preserve volume long-term and enable slow tissue remodeling. Advances here might help surmount limitations like a lack of donor fat and unpredictable resorption encountered with conventional fat grafting.
4. Clinical Evidence
Direct clinical evidence for synthetic fat grafts is limited in context. As a point of comparison, autologous fat has recorded one year survival rates in the range of 50 to 70 percent. Until strong trials document long term durability and safety with synthetic grafts, remarks about superiority are tentative.
5. Patient Experience
Synthetic grafts might shorten recovery by eliminating donor-site procedures and lessen scarring. Controls and predictable volumes may make everyone happier.
Patient feedback would probably emphasize fewer operations and more stable results, but long-term studies are necessary.
A New Paradigm
Synthetic fat grafting is a new paradigm in the way clinicians think about soft tissue augmentation and reconstruction. Conventional fat grafting depends on liposuction to obtain autologous fat. Synthetic grafts employ engineered substances intended to simulate the volume, consistency, and bio-behavior of native adipose.
This changes technique and logistics: no donor-site surgery, shorter procedure times, and supply that is consistent from batch to batch. That consistency is important because one significant limitation of existing fat grafting is inconsistency in graft survival, with approximately 50 percent to 70 percent of transferred cells surviving the critical three to six months vascularization period.
Synthetic grafts seek to bridge that gap by offering both predictable scaffold characteristics and defined resorption profiles. The applications for soft tissue work will expand as synthetic alternatives advance. Facial rejuvenation can employ small, well-shaped synthetic implants to substitute volume lost with age, minimizing harvesting even in thin patients who today are candidates only for small-volume transfers.
Body contouring and breast reconstruction are likely next. Synthetic grafts can be made in larger volumes without the trade-off of donor-site sculpting limits. Trauma or cancer reconstructive surgery could take advantage of sterile, off-the-shelf materials that are immediately available and standardized between centers, assisting in urgent or staged procedures where timing is often a critical factor.
We would expect synthetic grafts to supplant liposuction-based harvest in most procedures. Liposuction has its advantages as it shapes a donor site while providing graft tissue, but it contributes to operative time, expense, and theoretical morbidity. Regulatory frameworks already permit autologous fat transfer under minimal manipulation, and safety data are encouraging: a 2023 systematic review found no elevated cancer risk from autologous fat transfer.
As synthetics collect similar safety profiles and biocompatibility data, clinicians and patients may opt for avoiding another surgical site. A shift to synthetic grafts would normalize the outcomes and minimize the variability in graft survival. These engineered matrices can be tuned for pore size, degradation rate, and integration cues to favor vascular in-growth and long term volume maintenance.
Standard lots and validated processing minimize the batch-to-batch variability that presently results from harvest method, centrifugation and handling. Global practice patterns differ. Asia has adopted fat grafting aggressively for facial work, while Europe and North America divide facial and body demand.
Synthetic grafts provide a standardized product clinicians can leverage worldwide, expanding access and consistency. Pragmatic adoption steps are comparative trials, head-to-head safety studies, and train-the-trainer programs to standardize technique and aftercare.
The Human Element
Synthetic fat grafts alter the medium, not the human expertise and experience at the heart of treatment. Surgeons still need to position grafts with a precise strategy in order to achieve the optimal natural shape and prevent lumps or contour abnormalities. Proper graft placement means knowing your tissue planes and blood supply and how different areas age.
Even with uniform synthetic grafts, the clinician determines thickness, stratification, and how to meld the graft with local tissue. These decisions are significant for discretely effective outcomes that many patients today desire, particularly younger groups who want minimal adjustments of a natural sort as opposed to big, bold transformations.
Patient selection and surgical planning are still key. Not every candidate is a good fit for synthetic grafting or autologous fat transfer. Screening covers medical history, skin quality, smoking, and realistic goals. It plans where grafts go, how much volume to use, and if staged procedures are needed.
In reconstructive cases following tumor resection or injury, the strategy needs to consider scar tissue and irregular vascular beds. With facial augmentation, the strategy has to account for the way facial fat changes with age. Protocols need to be personalized. A generic dose has the potential for overcorrection or underfill and impacts long-term stability.
It needs to be nuanced and even-handed. Explain differences between synthetic and autologous fat. Autologous fat is biocompatible and lowers allergy risk because it uses the patient’s own tissue, and it has a long history dating back to the late 19th century.
Remember, approximately 50 to 70 percent of transferred fat typically survives long term, but swelling can linger for weeks and complete stabilization can take months. Be clear about risks. Graft necrosis can occur where adipocytes lie more than about 2 millimeters from a blood source, and both techniques carry infection, asymmetry, and need for revision.
Establish expectations on longevity, recuperation, and probable touch-ups. Use metric measures of volume in planning and in clear time frames of healing.
Training and curriculum changes will determine how effectively surgeons embrace synthetic grafts. Fellowships and residency programs need to add hands-on modules for synthetic products, training on how to blend synthetic grafts with native tissue, and simulation for placement techniques.
Trainees need exposure to reconstructive and aesthetic cases to see how graft survival, vascular supply, and tissue handling vary by indication. Add outcome tracking and patient reported measures to optimize protocols. As demand for cosmetic procedures grows worldwide, skilled surgeons are crucial to deploy new materials safely and fulfill patient expectations.
Regulatory Hurdles
Synthetic fat grafting encounters several regulatory obstacles that dictate the manner and timing with which it may supplant liposuction-harvested autologous fat. Present obstacles encompass modest clinical uptake, as merely 12.8% of physicians employ fat transfer extensively, mirroring regulatory prudence and inconsistent data. Fat transfer dates back to 1912. Early complications and vague standards stymied progress.
Today regulators need definitive clinical evidence that a synthetic counterpart equals or improves upon autologous fat in safety, durability, and patient outcomes before widespread approval. Regulators want standardized testing and long-term safety data. Devices and materials need to demonstrate the uniformity of their composition, sterility, and actions post-implantation.
This means reproducible manufacturing runs, validated assays for particle size or scaffold degradation, and batch-level quality control. Long-term follow-up studies are critical. Regulators are looking for complication data around fat necrosis, which accounts for 62% of reported fat grafting complications, and asymmetry, which accounts for 14.4%, as well as more severe events, which account for 10.9%.
Without multi-year safety and efficacy data, agencies are unlikely to approve widespread clinical use. The manufacturers have some steps to go through for FDA or international approval. These include the traditional routes of preclinical proof of concept and safety in relevant animal models, followed by phased human trials collecting safety and efficacy endpoints.
Regulatory submissions require clear primary outcomes, definitions of complications, and follow-up care for monitoring and managing postoperative issues. For the FDA, devices could be 510(k) if substantially equivalent to a cleared device or PMA for novel implants. Biologics or cell-based components, such as ASCs, introduce another layer of complexity as they typically become regulated as biologics, involving more CMC documentation.
There are 112 ASC-related trials ongoing, indicating strong research interest while representing additional regulatory hurdles. Regulators need full-fledged informed consent and risk disclosure. Practitioners need to give patients transparent information on advantages, side effects and the necessity for ongoing care.
This is important as patient appetite for natural, permanent volume restoration stays strong while regulators restrict some methods until they have more information.
Potential barriers to adoption include:
-
Insufficient long-term clinical data on safety and durability
-
Expensive regulatory trials and CMC
-
Classification ambiguity (device vs biologic) complicating approval path
-
Risk of fat necrosis and other complications brings regulatory scrutiny
-
Need for standardized outcome measures and imaging protocols
-
Variability in international regulations slowing global rollout
-
Reimbursement uncertainty and limited practitioner training
Future Outlook
Fat grafting occupies an intersection between regenerative medicine, tissue engineering, and patient desire. Active research in these areas indicates continuing progress in the manner in which artificial fat grafts will be created, manipulated, and applied. Enhancements will arise from superior scaffold materials mimicking native adipose mechanics, optimized microarchitecture encouraging vascular in-growth, and fabrication producing uniform particle size and purity.
As lab techniques advance, anticipate more consistent grafts that endure the transfer and are reliable once implanted. Stem cells and bioactive factors will come in the next wave. Providing adipose-derived stem cells with the graft or infusing growth factors in a scaffold promotes faster blood vessel formation and fat cell survival.
Real-world examples might be soft co-culture of stem cells with adipocytes prior to grafting or slow release gels that release vascular growth factors over weeks. All of these strategies hope to push durability well past the usual 50 to 70 percent ranges, minimize the need for retreatment, and decrease early bulk loss that necessitates a second treatment at three to six months.
Wider clinical applications will arise as the biology becomes clearer. Synthetic grafts could be tuned for nerve-bed support in reconstructive nerve work or formulated to expedite closure and tissue quality in chronic wounds. In breast reconstruction and natural breast augmentation, cultured fat might deliver a safer alternative to implants for some patients, supplying tissue that ages with the body and fluctuates with weight gain or loss.
In periorbital work, more predictable synthetic grafts might make under-eye hollow correction and dark-circle improvement persist and diffuse more reliably over the months it takes real results to emerge. Safety and predictability will fuel adoption. Less invasive harvest-free techniques lower donor-site hazard and streamline procedures.
Standardized prep and QC will eliminate variability observed with today’s autologous fat transfers and standardize results across clinics worldwide. Regulators and payers will observe data regarding durability, reoperation rates, and complication profiles. Promising data may broaden indications and drive increased adoption.
Where this gets us is a slow transition, not an overnight exchange. Fat grafting remains common, particularly where patient-supplied tissue is favored. Synthetic alternatives will flank it, preferred where harvest is unfeasible or where synthetic characteristics provide distinct medical benefits.
Clinicians can anticipate new tools, schedule different follow-up timelines as grafts settle over months, and counsel patients about probable retention, aging with the grafted tissue, and potential touch-ups.
Conclusion
Synthetic fat graft future replacing liposuction harvest Trials indicate less donor discomfort, quicker recuperation, and more stable volume over time. Initial products mimic native fat in touch and performance in laboratory and animal testing. Small human studies are encouraging, but there is no large, long-term data. Regulators want defined safety markers and reproducible manufacturing processes. Patients will care about cost, access, and visible results. Clinicians will observe typical integration and minimal complications. Now, investors and makers must think about straightforward, hard-nosed trials and transparent supply chains. Anticipate slow improvements, not an overnight replacement. Watch new trials and approved regulated approvals to see when synthetic grafts transition from promise to standard use.
Frequently Asked Questions
What is synthetic fat grafting?
Synthetically fat graft future replacing liposuction harvest. They seek to substitute or augment patient-derived fat and minimize liposuction-based harvest.
How does synthetic grafting compare to traditional fat transfer?
Synthetic grafts ditch donor-site surgery and speed recovery. They provide uniform volume and less variability, but long-term results and integration may vary from living fat cells.
Are synthetic grafts safe?
Early clinical data are promising, but safety hinges on the material, surgeon experience, and regulatory approval. Long-term studies remain needed to confirm durability and complication rates.
Will synthetic grafts fully replace liposuction harvesting?
Not yet. Synthetic grafts could eliminate the need to harvest in many instances, but autologous (patient’s own) fat may still be favored for certain applications based on results and patient preference.
What regulatory hurdles exist for synthetic fat products?
The makers will have to demonstrate safety and efficacy to regulators. This means clinical trials, manufacturing standards, and post-market surveillance that can take years.
How soon could synthetic grafts become widely available?
Its availability hinges on clinical trial outcomes and regulatory green lights. Others are in early clinical use. It could be years before it sees widespread adoption as the evidence mounts and regulators move.
Who is a good candidate for synthetic grafting?
Potential candidates are those seeking volume restoration who want to steer clear of donor-site surgery. Ultimately, it depends on your medical history, objectives, and your surgeon’s evaluation.


